We aim to help treat and manage your symptoms and pelvic health concerns. We also work to support carers ensuring that they have the right advice and support to help manage symptoms.
We are NOT a pad service, we will always prescribe treatment options first and if you require containment products we can prescribe to meet your evaluated clinical needs.
Our service covers adults over the age of 18 years and children and young people with complex needs (North of the county only) who are registered with a GP in Staffordshire.
We understand that this is a very sensitive area and our team are well used to putting people at ease, helping discuss your concerns in an open way.
Treatment plans may include:
Pelvic floor re-education
Bladder and Bowel re-training
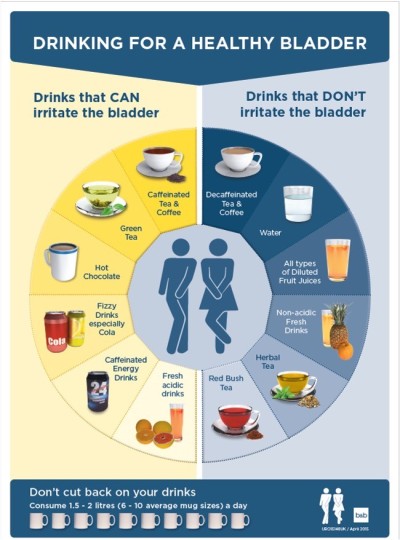
Healthy dietary and Fluid advice – to reduce irritation to the bladder muscles and improve bowel health.
Electrical stimulation to promote muscles activity
Catheter care management and problem solving of catheter associated issues
Teaching Intermittent Self Catheterisation
Containment products to help manage symptoms where appropriate.
We will liaise with your GP or consultant about medication as required and will refer clients to see a hospital consultant if necessary.
We also work closely with other teams throughout MPFT and the wider health community to ensure the correct training, advice and support are available to manage conditions, symptoms and concerns.
For telephone support, please call 0300 123 0901 and press option 1.
We accept referrals from:
GPs, consultants and any health care professional (on appropriate referral form)
We will either offer you a telephone, video consultation or clinic appointment initially. You will be asked several questions about your problems and your medical and social history.
It would be helpful to have a think about the answers to these questions before you attend:
What part of this problem bothers you most?
How and when did your symptoms/condition start?
Are there any activities or positions that make your symptoms better or worse?
How often during the day and night do you need to empty your bladder and bowel?
How much and what type of fluid do you drink each day?
Have you had any tests or investigations already for your condition?
What medications are you taking?
Depending on your symptoms these are some charts that may be helpful to complete to give more idea of how your symptoms bother you.
If your problems are related to your pelvic floor, an internal examination is often advised to assess your pelvic floor function and to fully understand where the issues are arising from. This can be completed at the first or subsequent appointment. We will discuss with you what it involves and why we feel it would be helpful for diagnosis and to help improve your outcome. You do not have to have this examination and have the right to change your mind at any point. If you would like a chaperone in your consultation or treatment, please let us know.
Finding out all this information helps us advise you on what the best treatment and management options are possible. To get the most from treatment we will ask you to follow advice and do exercises at home.
Subsequent appointments
We will review what advice and exercises you have been given and find out how your symptoms / problems have responded. We will progress exercises as we can and offer you further advice to improve your symptoms.
Following assessment and treatment we do have the options to liaise with your GP or consultant about medication as required and refer back to your GP or onwards to the consultants for further treatment.
Bladder dysfunction is a term used for a range of problems with the way the bladder holds and releases urine. We should be able to hold good volumes of urine in our bladder, get calm messages to empty, make it to the toilet on time, and fully or nearly-fully empty our bladder with ease.
Unfortunately when one or more parts of this don’t work as they should, this can become a very embarrassing problem.
Stress Incontinence: Leaking caused by an increase of pressure on the bladder such as when you cough, sneeze, laugh, move or lift.
Urgency: A strong desire to get to the toilet, not necessarily with a full bladder. Often with turning on the tap, on putting the key in the door or on seeing the toilet.
Urge Incontinence: leaking following a strong desire to reach the toilet and ‘not making it on time’.
Mixed Incontinence: both symptoms of stress and urge incontinence.
Frequency: going to the toilet too often i.e. more than the maximum of eight times in a 24 hour period.
Functional Incontinence: due to restricted mobility you may finds it difficult to make it to the toilet on time or can’t get undressed quickly enough to use the toilet without leaking.
Self Help Tips
Ensure you drink a good amount of fluid: approximately 1.5 - 2 litres of fluid per day
Stop drinking or take only small sips 2-3 hours before going to bed but make sure you still drink 6-8 glasses of fluid each day (try sucking ice cubes or ice lollies)
Reduce or remove caffeine and fizzy drinks from you diet, especially in the evening
When you need to go to the toilet, try not to panic and rush to get there
Make sure you empty your bladder properly, sit down rather than crouching over the toilet
Rock back and forward after going to the toilet to fully empty (i.e. double void)
Sitting in a good posture allows you to stand up with less effort, which can reduce leaking
Train your pelvic floor muscles and get them working before you cough or sneeze or as you walk to the toilet
Stop smoking: smokers are 1.5 times more likely to have an overactive bladder due to the effect of nicotine
Elasticated waist bands are easier to manage in a hurry.
For men:
Double voiding: sit down (if you normally stand to pass urine) or stand up (if you normally sit to pass urine), count slowly to 20 and sit back down or stand back up and attempt to urinate again.
"Milking" - pushing the last few drops of urine from the penis with your fingers by pushing up just behind the testicles, before the final shake.
Ask your GP for advice as this might be related to your prostate.
Bowel dysfunction refers to the inability to control bowel movements, including problems with the frequency and consistency of bowel movements. These symptom can be a source of upset and embarrassment, as well as discomfort.
What is Normal?
having a poo as often as 3 times a day to 3 times a week
poo should be moist and well formed (not too hard and lumpy and not too soft and mushy)
It should be easy to pass without straining or pain
you should feel empty afterwards
Loss of bowel control
This may show in a variety of ways:
Leakage of stool: symptoms involve staining in pants or leakage on way to toilet
Leakage of mucus: passive leakage in pants without noticing
Inability to control flatus: flatus escapes easily with movement
Urgency of stool: having to run to toilet as soon as you feel the urge and sometimes without making it in time
Difficulty cleaning: having to go back and wipe repeatedly
Further Defecation Disorders
Chronic Constipation
Symptoms can be:
You have to strain a lot to poo
Your poos are hard and lumpy
You feel unfinished after having a poo
You feel bloated, stomach pain and discomfort
Your poo less often than is usual for you
In some cases:
You may have a bad taste in your mouth, bad breath, decreased appetite, lethargy.
Passing foul smelling wind
Leaking of liquid or loose stools. When large stools get stuck and block the bowel, liquid stool can pass the blockage.
Causes of constipation
Not drinking enough fluid
Not eating enough fibre
Putting off going to the toilet
Not moving enough and spending long periods of time sitting or lying in bed
Not exercising
A side effect of medication
Changing your daily routine or diet
Some neurological problems such as Parkinson’s Disease and Multiple Sclerosis
Difficult emptying the bowel, which may or may not be associated with constipation.
Irritable Bowel Syndrome (IBS)
Self Help Tips
Ensure you drink plenty of fluid to avoid constipation (1.5 - 2 litres of fluid)
Caffeine, fizzy drinks and sweeteners may irritate your bowel making you more loose
Don’t ignore the need to empty your bowel
When you need to go to the toilet, try not to panic and rush to get there
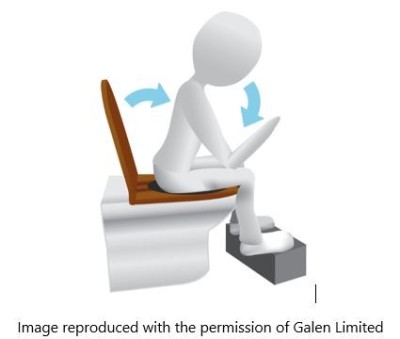
Sitting position on the toilet is really helpful
Ideally knees should be higher that hips
Lean forward with a straight back
Avoid straining
Do not hold your breath, try to breath out as you let go
Using a clean hand, supporting underneath (on your perineum) or use a finger or thumb against the back wall of the vagina, can be helpful to fully emptying your back passage
Train your Pelvic floor muscles and get them working when you feel the urge
Elasticated waist bands are easier to manage in a hurry
Children and young people from the age of 4 - 19 years who live in Staffordshire. At the age of 18 the young person would transition over to the care of the adult service.
How do I refer?
GPs, Paediatricians, Social Workers, Health Visitors, School Nurses, or Community Children's Nurses, or any other professionals working with the family, who have obtained appropriate consent can refer by completing the referral form and emailing spht@mpft.nhs.uk.
We will make a link with the child or young person's school if needed and advocate for the needs to be met whilst they are attending school. We can provide school staff with education / training and support with care planning. We will also offer home visits.
We deliver one Children's Specialist Clinic for Bladder and Bowel Dysfunction per month for children and young people who live in the City of Stoke on Trent, Staffordshire Moorlands or Newcastle under Lyme.
This is held on Friday 9.00 am - 12.00 pm at Ryecroft Health Centre, Broad Street, Newcastle, ST5 2BQ.
Following our assessments we may refer on to other services such as Pediatrician, Urologist, GP, School Nurse, Health Visitor, Gastroenterologist, CAMHS learning disability team, and the Children's Community Nursing Team, and constipation clinic.
Menopause is a natural part of every woman's life and isn't always an easy transition for all, but with the right support it can be much better.
'Meno' meaning 'menstrual cycle'
'Pause' meaning 'stop'
Officially you are not menopausal until you haven’t had a period for a year.
As women get older their ovaries don’t work quite as well and stop producing as much of the sex hormones oestrogen, progesterone and testosterone. An egg is no longer released every month and periods start to change in nature and frequency. Usually they start to become less frequent and can take months or years to stop completely.
Sometimes periods stop very suddenly, where ovaries are removed in surgery or after other gynae surgery. Also chemotherapy or radiotherapy to the pelvic area can affect how ovaries work.
This normal decline in oestrogen occurs between the ages of 45 and 55 years of age. In the UK, the average age for menopause is 51.
1 in 100 women under the age of 40 have an early menopause and 1 in 1000 under the age of 30.
Perimenopause
is the time leading up to menopause where you experience menopause symptoms but are still having periods. Periods change, becoming further apart or closer together and can be more irregular and the flow can change becoming heavier or lighter.
Symptoms of Menopause
Symptoms can occur months or years before your periods stop and last around 4 years after your last period. Most women will experience symptoms with the common ones including:
Hot flushes
Night sweats
Vaginal dryness and discomfort during sex
Difficulty sleeping
Low mood or anxiety
Reduced sex drive (libido)
Problems with memory or concentration
Genitourinary Syndrome of Menopause
This was previously known as vaginal atrophy or atrophic vaginitis.
The name has changed to recognise that it is not just the vagina that is affected by the reduction in oestrogen. Changes also occur to the clitoris, labia, bladder and the urethra, the tube running from the bladder to the outside.
Vagina and vulva symptoms
The vagina is the muscular canal travelling from the outside of the body to the womb
The vulva refers to all the external sex organs, including the labia, clitoris and vaginal opening.
Lacking oestrogen affects the walls of the vagina and the vulva. They become thinner and have less stretch meaning they are more susceptible to injury. Also a lack of oestrogen changes the vaginal fluid. It becomes thinner and less is produced causing the symptoms below.
dryness (up to 75% of women experience this)
irritation and itching
burning and discomfort
discharge
more at risk from infections and inflammation
Treatment Options:
Vaginal moisturisers and lubricants
local oestrogen replacement gel or pessaries
Urinary symptoms
The changes in hormones affect the bladder and urethra, the tube from the bladder to the outside.
Symptoms may include:
Recurrent urinary tract infections (UTIs) - occur in 20% of females
Over active bladder symptoms - urinary frequency and urgency and urge incontinence. (Stress incontinence also possible)
Pain with emptying your bladder
Leaking a dribble after going to the toilet
Wakening at night to need to go to the toilet
Blood in the urine
Self Help Tips
Ensure you drink a good amount of fluid: approximately 1.5 - 2 litres of fluid per day
Stop drinking or take only small sips 2-3 hours before going to bed but make sure you still drink 6-8 glasses of fluid each day (try sucking ice cubes or ice lollies)
Reduce or remove caffeine and fizzy drinks from you diet, especially in the evening
The pelvic organs (bladder, womb, vagina and bowel) are supported and kept in place by the pelvic floor muscles and surrounding tissues. Sometimes these muscles and tissues develop problems and one or more of the organs may no longer sit in the ideal position and droop. They may bulge into the vaginal canal or even externally. This affects about one third of women over their life time.
It is thought that the stability of the support to the pelvic organs may be affected by a reduction in oestrogen.
There is a link with increased BMI and waist circumference and pelvic organ prolapse. Post menopausal women have a tendency to carry more weight around their abdomen.
Self Help Tips
Limit heavy lifting where you need to strain. Avoid holding your breath. Lifting from ground level is harder than from waist height.
When it can’t be avoided, before lifting, engage your pelvic floor muscles. Lift with a good posture.
Do not hold your breath, try to breath out as you let go
Support underneath using your hand or a finger or thumb internally, to help you empty your bowels
Rock back and forward after going to the toilet to fully empty. i.e. double void.
Maintain a healthy weight
Strengthen your pelvic floor muscles, this may be easier in lying initially.
If feeling particularly heavy, lie down, knees bent, with a pillow under your bottom to allow gravity to reduce the heaviness. Do some pelvic floor exercises in this position.
Exhale with every effort. Never hold your breath or pull your tummy in strongly during an exercise.
The muscles of the pelvic floor cause problems when they weaken but they can also cause problems when they overwork and have difficulty relaxing. When these muscles spasm, blood flow decreases and there is a build up of lactic acid. This will cause pelvic pain.
Vaginismus
Vaginismus is a condition where the pelvic floor muscles suddenly become so tense that to try and insert something into the vagina is impossible or very painful. It is a very distressing condition.
Often there's no obvious explanation, but some things thought to cause vaginismus include:
fear that your vagina is too small
a bad first sexual experience
an unpleasant medical examination
a belief that sex is shameful or wrong
a painful medical condition, like thrush
Treatment usually focuses on:
managing your feelings around penetration
exercises to gradually get you used to penetration
We work with you, at a pace you are comfortable with, to fully relax your pelvic floor muscles and have better control over them. With gentle squeezing we can gain better relaxation, breathing and visualisation exercises and through gentle touch we can aim to fully relax the pelvic floor.
The Pelvic Floor muscles are a group of muscles that form a hammock at the bottom of the pelvis.
The Pelvic Floor Muscles Role is to:
Control the bowel and bladder, allowing them to empty and preventing leaks
Support everything in your pelvis, preventing prolapse
They have a role in sexual function
What causes pelvic floor muscle weakness?
Pregnancy and Childbirth
Hormone changes of menopause
Being over weight
Decreased muscle tone with ageing
A chronic chough
Long term straining when constipated
Repeated heavy lifting
Pelvic surgery
Inactivity
How to do pelvic floor exercises
Pelvic floor exercises can be done anywhere and anytime, but initially you may prefer to do them in sitting or lying.
Lie or sit comfortably with your knees slightly apart and feet flat on the bed or floor
Tighten and pull up the ring of muscles around your back passage, as if you are trying to stop passing wind (don't tighten your buttock or thigh muscles while you do this)
Also tighten and pull up the muscles around your front passage, as if you are trying to stop passing urine.
Keep breathing!
There are two types of exercises: Slow Twitch and Fast Twitch.
Slow twitch muscles are endurance muscles and help keep everything in a good place all day.
Fast twitch muscles respond quickly when needed e.g. with coughing, sneezing and running.
To perform the slow twitch exercises:
Count how long you can hold the squeeze (maximum 10 sec).
Relax and let go for 10 sec.
Repeat for a maximum 10 times or until you muscles feel tired.
To perform the fast twitch exercises:
Pull up the pelvic floor muscles as before.
Hold for one second and then relax.
Repeat for a maximum 10 times or until you muscles feel tired.
It is important to try not to:
Squeeze your buttocks together
Bring your knees together
Hold your breath
Pull in your tummy muscles too much
Lift your shoulders / eyebrows or toes upwards.
If you do any of these, you are not working your muscles correctly.
How often should I practice?
Try and build your pelvic floor exercises into your everyday life. e.g. after going to the toilet and while brushing your teeth.
Constant repetition gets good results. Always work your pelvic floor muscles before you cough, shout, sneeze, jump or lift, or anything that makes you leak.
If you find it is a panic to go to the toilet, work your pelvic floor to delay going and as you walk to the bathroom.
Once you feel confident in doing the exercises try doing them in all positions, such as standing or walking.
How quickly will I see results?
Your muscles can take up to 6 weeks to get stronger, but you may notice improvements sooner if you start getting your muscles to work before things that cause you a problem e.g. coughing / sneezing. It may take up to 6 months to see a significant improvement.
Do not give up! Pelvic floor exercises have been shown to give great results when you continue doing them for life!
The pelvic organs (bladder, womb, vagina and bowel) are supported and kept in place by the pelvic floor muscles and surrounding tissues. Sometimes these muscles and tissues develop problems and one or more of the organs may no longer sit in the ideal position and droop. They may bulge into the vaginal canal or even externally. This affects about one third of women over their life time.
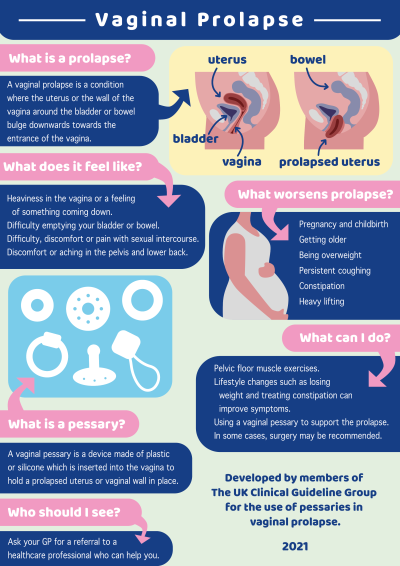
What are the symptoms of vaginal prolapse?
You could have one or more of these symptoms
a feeling of something coming down, a dragging sensation or a bulge in the vagina
difficulty emptying your bladder or bowel
discomfort / pain during sexual intercourse
discomfort or aching int eh pelvic and low backache
What causes pelvic organ prolapse?
Anything that puts increased pressure on the abdomen can lead to pelvic organ prolapse including:
Pregnancy and childbirth
Getting older
Being overweight
Respiratory problems with a chronic long term cough
Constipation
After a hysterectomy (surgical removal of the womb/uterus)
Heavy lifting
Genetics play a roll
Some of the most common vaginal prolapse:
Anterior vaginal prolapse: where the anterior vaginal wall does not adequately support the bladder. This can make it difficult to fully empty the bladder, increasing risk of urinary tract infections, and can lead to an increase in symptoms of urgency
Posterior vaginal prolapse: the posterior vaginal wall doesn’t adequately support the bowel. This can make it difficult to initiate emptying or fully empty with ease
Uterine prolapse: the cervix and uterus descend into the vaginal canal
The rectum can also prolapse through the back passage (rectal prolapse).
Self Help Tips
Limit heavy lifting where you need to strain. Avoid holding your breath. Lifting from ground level is harder than from waist height.
When it can’t be avoided, before lifting, engage your pelvic floor muscles. Lift with a good posture.
Do not hold your breath, try to breath out as you let go
Support underneath using your hand or a finger or thumb internally, to help you empty your bowels
Rock back and forward after going to the toilet to fully empty. i.e. double void.
Maintain a healthy weight
Strengthen your pelvic floor muscles, this may be easier in lying initially.
If feeling particularly heavy, lie down, knees bent, with a pillow under your bottom to allow gravity to reduce the heaviness. Do some pelvic floor exercises in this position.
Exhale with every effort. Never hold your breath or pull your tummy in strongly during an exercise
What is a Vaginal Pessary?
It is a silicone or plastic device, which is inserted into the vaginal to hold a prolapse uterus or vaginal wall in place and support your bowel and bladder. Once correctly fitted it may help to reduce your symptoms and make you feel more comfortable. There are different types of pessary and it can take more than one visit to get the right size, fit and type for you.
If appropriate you may be prescribed products to manage your incontinence based on your clinical need. Prior to a full delivery we will ask you to try sample products to assess the suitability of them.
Re-ordering Info:
Call 0800 085 4907 to reorder.
Two weeks prior to when you are due your first re-delivery, you will receive a ‘Welcome to Tena’ letter, which will have all the order information you need.
MPFT’s Specialist Pelvic Health Team empower male patients to dispose with dignity
“Embarrassed, stressed and isolated” - three words used by one man with incontinence caused by his treatment for prostate cancer to describe how he feels every single day. Men who need to dispose of their sanitary waste often have no direct access to a sanitary bin in male toilets.